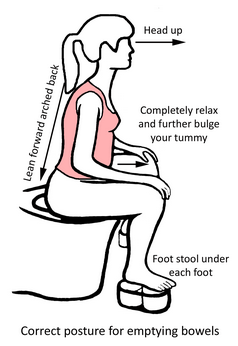
 Uncomfortable conversation? Toileting is an activity that we engage in about 10x per day and, yes, it's private but it's still important to talk about! There are good and bad ways to spend your time on the toilet and some of them depend on your particular body, your particular resting and active tone, patterns of movement and breath and the health of your digestive system. It depends on whether or not you've had surgery, have scar tissue, are rushing, have privacy, how you were taught about toileting as a child….so many factors. Let's start with "normals": It's normal to void (release your bladder, urinate or pee) 6 - 8 x per day, including night time voids. You shouldn't be voiding at night unless you're over 60 and then only once. After 80, twice is acceptable. You should never need to rush and you shouldn't leak en route. You should also be able to tell your bladder to wait. Traveling to the toilet to void every 3 ½ to 4 hours in a calm, controlled and easy manner is awesome. You should enjoy a painfree exit of clear unscented urine and never needing to push or be effortful. It should take 15 - 18 seconds and be in a Bell Curve, starting slow, building to a crescendo and ending with ease. There should be no post-void dribble, no double voiding…..wipe and go dry until next time! It's normal to empty your bowels (BMs or pooping) 1 - 3x per day up to every 3 days. Optimum is a full, complete and satisfying BM soon after waking up/eating your breakfast. Again, you shouldn't need to rush, but you should pay attention to the nudge to go to the loo for your morning BM. Don't ignore it and don't delay it. Spend 5 - 10 minutes enjoying bowel release. Toilet position for bowel release is seated comfortably, with support, either in a slouched posture or with your elbows on your knees as if you're reading a newspaper on the floor. The posture that's just right for you is dependent on the angle of the Puborectalis muscle that slings around the Anorectal Canal. Are your knees slightly higher than your hips with a raise under your feet? Squatty Potties are trendy, but for some people they raise the knees too high, tightening up their pelvic system making release of BMs more difficult. In addition, the consistency of your BMs matters. If you have loose, liquidy BMs (5 to 7 on the Bristol Stool Chart), the message that your internal anal sphincter sends to your brain when stool lands in the rectum is "Run!". If you have normal BMs (3 and 4), the message will be a calm nudge, "It's time now." If you have stodgy, dried out stool (1 and 2), the message gets distant…..it's your job to waken it up and pay attention to the faraway call, "It might be time soon.". You can waken this up with gentle heat on your lower tummy and belly massage upon awakening/during breakfast. This doesn't move stool along the passageway, but it does awaken peristalsis, the gentle squeezes that move stool through the colon. Having a tap-hot glass of water at night while you do your last tooth brushing just before bed can keep your stool hydrated overnight. A shot glass (2 T.) of prune juice along with your water may help. Avoiding all dairy, especially cheese, can help some people, along with reducing meat and increasing nuts and beans. Increasing fibre needs to be applied with caution. Recent studies show that increasing your fibre (leafy green vegies, ground flax seeds, psyllium, whole grains) needs to be done in 10% increments per week. Too much fibre makes for sticky stool, making exit more challenging and wiping truly "a pain". Not rushing is important. Take time to breathe into your belly, teaching your pelvic floor to release, opening your anal sphincters, creating ease. If you're sensitive to sound, turn on the fan or music. If you're sensitive to smell, keep a candle/scented spray nearby. There is no one answer to happy toileting, but it pays in good longterm health to find yours!
0 Comments
The bossiest, most demanding part of our pelvis is our "back passage" (our anorectal function, BMs or pooping). If your bowels aren't emptying well (full, complete and satisfying daily BMs), then your bladder, your pelvic organ support, your intimate function and your general sense of wellbeing won't be thriving either. "Back Passage First" is a rule in pelvic physiotherapy. Once you learn and/or relearn wonderful bowel release, your other pelvic issues may be addressed with ease.
What is normal for your BMs? The rule is that you enjoy a full, complete and satisfying BM at least every 2nd or in rare people, every 3rd day or as frequent as 2 - 3x per day for some people. There should always be a sense of full evacuation of your stool, not a sense of "there's still some left behind". There should be ease in release, not pushing, forcing, breath-holding or grunting. There should be ample time to get to the toilet, not making a mad dash to get there in time. There should be a clean exit with tidy wiping with ease, no skid marks in your undies or loss of stool without you being aware. There should be no straining or pushing or pain. And it should end with a sense of satisfaction of a job well done! What should a normal bowel movement be? Perhaps surprisingly, we talk about this a lot and the smart folks in Bristol, England developed the Bristol Stool Chart. It's a handy guide to give both you and your health care providers a simple way to talk the same language about our bowel function. The scale goes from 1 to 7. Numbers 1 and 2 describe hard lumps, either separate or together…..think deer droppings and indicate a level of constipation. 3 and 4 are sausage-y like shapes, sometimes dry and cracked or smooth and snake-like. If your bowel movements look like 3 and 4, that's great as long as they're the width of a sausage, not a pencil. That indicates other issues. 5 is soft and blobby with clear edges and indicates a lack of fibre in your diet. 6 is the beginning of diarrhea, soft and blobby but with ragged, frayed edges. 7 describes full-on diarrhea….loose, watery, liquid poop with nothing solid visible. Understanding and getting familiar with the Bristol Stool Chart can help you describe to your health care providers what's going on inside you. It's not normal to have blood or mucous. Blood can appear from a hemorrhoid and enthusiastic wiping or can be an indicator that there are more challenging problems. Mucous shouldn't be in our digestive tract and suggests that your body is fighting an infection. You need to see your doc, either way. Your BMs should be brown, with no undigested food visible, not chalky or blackish or have a truly foul or different-from-normal odour. We're not talking smelling like roses, but healthy BMs don't smell awful! Stop and have a gander…..this is digested food that's done its job for you, feeding you and giving you nutrition, energy for your life and yumminess….be grateful and pay attention. Your BMs give you cues about your health. Your toileting habits matter. Firstly, it's important to understand the gastrocolic reflex. This is the nudge that you receive (thanks to your lower esophageal sphincter chatting with your lower colon) when you start your day with a warm, caffeinated drink. As you swallow, your colon gets the message, "Empty out yesterday's food…..today's is coming!" Paying attention at that moment will help you establish beautiful bowel habits. Go to the loo. Spend some relaxed time, not rushing, calmly breathing into your belly, with your knees slightly higher than your hips on support, massaging your tummy and enjoying effortless bowel release. It takes opening of the pelvic floor to accomplish this, so calm, unrushed presence is really helpful. Don't wipe right away. Take a few more breaths to be sure that you're done. Toileting habits will be in our next "chat". Bladders and bowels ask different things of us on the toilet, so clarity around the messages you receive and your response is important. Happy BMs! We've talked about diagnosis, treatment and lymphedema in the last 3 articles. Now let's move onto two common, manageable secondary outcomes of breast cancer, CRF and Cording, "the other stuff". These conditions are so common that every woman going through breast cancer needs to become educated on what they are and how to address them. Read on! Cancer Related Fatigue (CRF) is experienced by 70 - 100% going through breast cancer treatment. Women describe it as a whole-body tiredness that isn't relieved by rest or sleep. We think CRF is due to many factors, including the cancer itself, radiation, chemo and stress. It may come on suddenly, isn't associated with activities or exertion and may continue after treatment is over. The thyroid may become underactive especially if the lymph nodes in the neck have experienced radiation, causing increased fatigue by reducing your ability to metabolize. The combo of radiation and chemo may lead to anemia, increasing our fatigue by reducing the availability of oxygen in our blood. Our appetite may be reduced as well, making us less likely to eat nutritiously. Some medications that are prescribed during treatment may also cause fatigue. Then, there's our emotional health as we go through medical interventions and treatments, causing stress, fatigue and sometimes depression. We know that healthy lifestyle choices can hugely impact CRF. Energy conservation is important, wisely choosing where, when and what you'll in a day. Don't try to maintain your normal daily routines. Set gentler, kinder, more compassionate goals. The CRF Golden Rule is "Never Go Below 25% in Your Tank". If you feel fatigue coming on, recognize that you simply don't have a "reserve tank" on board. Stop at the first sign of fatigue, before you're depleted, or it may take days to recover. Talk with your doctor about your thyroid function and iron levels as you may need support in these areas. When eating is a challenge, choose only the most calorie dense, colourful and nutritious foods. One wise woman taught me that adding plain yogurt to her food made it more palatable as well as easier to chew, swallow and digest. Guard your sleep and rest time with dedication and ferocity! Recognize that you are in restoration and rebuilding mode. Exercise can help by cleverly changing your metabolism and giving you more energy. It's important to "start low and progress slow" and be consistent. An important proviso is that radiation treatment is a time to maintain rather than gain. Axillary Web Syndrome or Cording is another common outcome from breast cancer surgery and treatment, seen in between 20 to 80% of women; its incidence depends on what kind of surgery and treatment you've had. Cords look like a guitar string that pops up under your skin anywhere from your chest to your armpit, elbow, wrist or palm. Women often see it for the first time when they stretch to put on their seatbelt or coat. A cord is your lymphatic vessel tightened up. They "mate once for life" and don't heal, so helping them release and get back to work is important. If you have cording, you also have a raised risk for lymphedema down the road. Your breast cancer physio can help you reduce or lose cording with lymphatic manual therapy, myofascial release and gentle stretching. You can regain full lymphatic function, release your lymph vessels/skin tissue and find full spinal and arm movement in the mix! We began by introducing breast cancer, risk factors and how we find it. We went on to talk about surgery, radiation, chemotherapy and hormonal therapy. After all this medical intervention, we are still one in eight women in Canada, finding our way and living out the rest of our lives. What challenges may we still face? Hormonal Therapies may be recommended; these are longer term medication, called Tamoxifen or Herceptin (and others). These are medications that are taken over a period of 5 - 10 years depending on the type of breast cancer that you have, how soon it was diagnosed, and your menopausal status. They offer some protection from cancer returning. Lymphedema is a condition in which there is a reduction in the natural lymph flow somewhere in the body. After breast cancer surgery and/or radiation there may be an interruption of the lymph flow through its watershed. The lymph system's job is to support your immune system and to interact with your circulatory system; it should flow uninterrupted, like a river. During breast cancer surgery, the tumour and local lymph nodes may be injected with a tracer and some dye. The surgeon is then able follow the dye to see which lymph nodes may be communicating with your tumour and remove them. Once your lymph nodes have been impacted by surgery and/or radiation, you are at a lifetime risk of developing lymphedema. Your job is to pay attention to mild sensational changes of heaviness, density or tingling in the arm. Lymphedema can't be cured, but it can be managed and treated with manual lymph drainage, compression garments specially designed for you and excellent personal care. We used to use of a machine called a lymphopress. Although the lymphopress may reduce the volume of a limb, it also may cause tightening or hardening of the tissues over the long term. We've advanced in our knowledge and treatment, so prevention is the key! Lymphedema Risk Reduction Practices are your job on a daily basis. You will know when and where to advocate for yourself and to ask for help.
CV Advance October 2018 Breast Cancer 201
Breast Cancer 201…..the details after diagnosis. We discussed how we develop breast cancer and how we might find it in Breast Cancer 101. How do we understand the label on our diagnosis and how do we begin to sleuth through treatment options? After we've been told we have cancer, we need to become an instant expert. We have to make decisions based on the information that we're presented at each medical visit. I'm hoping this information will help us all learn now…..perhaps for ourselves or perhaps to compassionately support a woman that we know and love. Numbers and Letters… Each breast cancer has a name and a number and letter to help us understand the type, nature and potential spread of the disease. Stage 0means that there are atypical cells, but no spread of the cancer into the ducts, lobules or surrounding tissues. It's early and non-invasive and accounts for around 20% of all breast cancer cases. Ductal or Lobular Carcinoma in Situ are in this category. Stage 1means that the tumour is under 2 cm. and has not spread into the lymph nodes or outside the breast tissue. Stage 2 (A and B)means the tumour is 2 - 5 cm. and may include up to 3 lymph nodes but has not spread further. Stage 3 (A and B)means that the tumour is larger that 2 cm. and may include up to 9 underarm lymph nodes and, with B, may have spread into the skin, chest wall, muscles and ribs. Inflammatorybreast cancer is an aggressive type of Stage 3B cancer, which also involves a reddened, inflamed breast. Stage 4tells us that the cancer has spread beyond the breast, chest and lymph nodes outwards to distant organs. Recurrentbreast cancer is the name used when it has returned; it may appear in the breast or elsewhere in the body. Now what? How do we go ahead? Most women will choose some type of surgery, their choice dependent on their type of cancer, impact on recovery and long term prognosis. Surgery a "local" treatment, used to remove tumour cells, to inspect/remove lymph nodes and to reconstruct the breast. Lumpectomyis a breast-conserving surgery and the least invasive procedure. The cancer is removed, along with some adjacent breast tissue and associated lymph nodes. Most women choosing this option will also need radiation. Total Mastectomyinvolves the surgical removal of the breast and lymph nodes as needed but the tissue beneath the breast is left intact. This is the most common surgery used to treat breast cancer. Radical Mastectomyis less common now, involving removal of the breast, pectoral/chest muscles and all of the lymph nodes. Reconstruction Surgerymay be begun during the initial surgery or it may be delayed. It may involve silicone or saline (salt water) implants or tissue flap surgery. The latter, tissue flaps, may mean taking some of a tummy muscle, buttock muscle or a back/shoulder muscle to be transplanted over to form breast tissue. More commonly now, your surgeon may recruit some tummy fat and blood vessels, called a DIEP Flap Reconstruction. This reconstruction has a natural feel and look, ages more naturally but takes time and multiple medical visits over some months. Radiation is a "regional" treatment, by directing high energy rays in order to destroy cancer cells. It can be given externally or internally (called brachytherapy). Most of the side effects of radiation (wait for the next article for more on this!) can be minimized and are not permanent. Chemotherapyis a whole-body or "systemic" treatment in which drugs are given through an IV or by mouth when they travel through the bloodstream and impact cancer cells. It may take some months to complete a series of treatments. Hormonal/Targeted Therapiesare a second form of systemic treatment. Hormonal therapy is used to reduce the risk of cancer returning or to treat cancer that has come back or spread. It changes the hormonal impact on the breast or simply reduces our hormonal load. |
Archives
January 2024
Categories
All
|
 RSS Feed
RSS Feed
