 Strategies for Menstrual Health You'll have about 400 periods in your lifetime, so track them, learn about your experience and how to thrive before, during and after each cycle.
Try one idea at a time to learn what works best for you. You are unique as are your cycles. What looks like a good idea for me? Practical? Applicable? During, before or after my period begins?
Property of Full Circle Physiotherapy, updated July 2022, not to be copied without permission.
0 Comments
 Kegels or Pelvic Floor Muscle Training (PFMT)by Sue Croft Physiotherapist | Jun 5, 2022 | Prolapse and pessaries, Urinary incontinence, Women's Health | 0 comments
There has been some recent bagging of Kegels (aka pelvic floor exercises) on Instagram and other important sources of life information and seeing as Influencers only need a good PR team and some sassy photos to extend their reach into the millions, I thought I’d post a very quick, short blog to put the alternative, supportive argument to not ditch Kegels before it was too late. In Australia, we actually don’t tend to use the term Kegels much but as this new trend is saying to Ditch Kegels, I am using that term in this blog. I am immediately stating my natural bias, that as a pelvic health physiotherapist, I have a strong evidence-based opinion on the value of actually seeking a pelvic health physiotherapy consultation to internally examine (with your consent) the status of your pelvic floor muscles and to validate what your best treatment programme might be to help your ‘pelvic floor distress’. The important thing to understand is that PF exercises or Kegels are just one part of a Big Apple Pie of treatment strategies. What that means is that addressing all components of a programme will lead to an excellent outcome for improving urinary leakage or bladder urgency or obstructed defaecation or faecal incontinence or pelvic organ prolapse or pelvic pain – NOT just Kegels. Let’s briefly dive into what affects the pelvic floor muscle strength. The levator ani (pelvic floor) muscles are stretched by 1.5 to 3 times their normal length during a vaginal birth, depending on the size of the baby, the baby’s head circumference and the mother’s pelvic outlet. Structural damage can occur to the PF muscles by directly tearing the muscles partially or completely from their attachment on the pelvis (called levator avulsion), from micro-tearing within the muscles which can lead to overdistensibility of the muscles or nerve damage (by compression or traction) which causes temporary or permanent weakness of the muscles. Levator avulsion occurs in about 20% of all vaginal births and is strongly associated with: the age of the mother, (occurrence more than triples during the reproductive years from below 15% when the mother is aged 20 years, to over 50% at when aged 40 years) (1); long second stage of labour; posterior presentation of the baby; head circumference > 36cm(2); baby’s weight over 4kg and the use of forceps, but it can also happen in vaginal deliveries with no instruments. (3) A pelvic health physiotherapist can give you insight into the possible changes that have occurred to the muscles, but also encourage and focus on ways to regain strength through targeted strategies such as: education regarding the correct activation of the muscles, biofeedback, electrical stimulation to the muscles through a hand held machine, weighted cones and especially functional pelvic floor strength work through supervised exercise. Kegels or pelvic floor exercises can seem worthless or useless if you have sustained a significant injury from a vaginal birth because you can’t seem to make the muscles work and therefore Kegels lose credibilty if that is all that has been offered to the patient (who then may go on to become an Influencer). Pelvic floor muscle training (PFMT) is a well-researched treatment strategy which is one (important) aspect of any pelvic health management plan, but may be completely inappropriate as a “one treatment fits all” package – particularly if a woman’s main complaint is pelvic pain. In fact if you have pelvic pain, you may be asked to focus on relaxing your pelvic floor (and tummy) muscles and avoid Kegels until the pain has resolved. So what are ten quick points to pay attention to when performing Kegels or pelvic floor exercises? • Do not hold your breath at all. Learn to breathe normally as you do any exercise. This is very important. Learning to exhale on effort will protect your pelvic floor rather than holding your breath. • Do not try too hard at first and stop if you sense any pushing down or bulging around the vagina. Check this by feeling with your hand. This is called ‘bearing down’ and can make your prolapse or incontinence worse if you continue. • It’s all about the timing and endurance of the muscles not just strength. If you have had nerve damage or muscle avulsion then we cannot cure that at this point in time. So if your muscles are very weak, then it is imperative that you recruit and strengthen what is available to you at the correct time. • Use reminders for your exercise session: Perhaps use coloured stickers around the house to remind yourself, or when you clean your teeth, turn on the kettle or whenever you walk through a doorway. If you have poor sensation and difficulty in recruiting the muscles, then it is best to do your exercises in a quiet room, in a very focused way, so you are sure you are doing the exercises correctly. Using an image of the pelvic floor muscles will get your brain involved and remember you do not have to get on the floor to exercise these muscles! • Remember to brace or engage before effort. Gently draw in your pelvic floor muscles before and as you cough, sneeze, lift a weight (especially toddlers), get out of bed or a chair, and anything that is strenuous. It will become a life-long habit or ‘knack’. • Relaxation of your tummy and pelvic floor muscles is very important especially if you have any pelvic pain. Balance all tightening with plenty of relaxation. • Move so you decrease strains on your body. When getting out of bed move through your side; divide heavy loads into smaller parcels; be aware when picking up toddlers (especially in the early days after a new baby); and teach young children to be independent to minimize lifting them. • Regular pelvic floor muscle training is for life and can improve stress incontinence and severity of prolapse. Incorporate these exercises into your activities of daily living. • Allow time for improvement and ensure all strategies become life-time habits. • These strategies are for life! 3 monthly phone diary prompts to remind you of all those strategies. And NUMBER 10: Once you have sorted your bladder, bowel or prolapse issues consider having a review from a pelvic health physiotherapist yearly. This way you will get on to any deterioration in function early. References: (1) Dietz HP (2009). Pelvic Floor Assessment. Fetal and Maternal Medicine Review, 20(1), 49-66. 10.1017/S096553950900237X. (2) Rostaminia G, Peck J, Van Delft K, Thakar R, Sultan A, Shobeiri SA (2017) New measures for predicting birth related pelvic floor trauma Female Pelvic Med Reconstr Surg 22(5): 292-296 (3) Dietz HP (2013). Pelvic floor trauma in childbirth. Australian and New Zealand Journal of Obstetrics and Gynaecology, 53(3), 220-230. 10.1111/ajo.12059. (4) Sue Croft (2022) Pelvic Floor Essentials book  Find Your Own Body…..How to Feel Your Own Pelvic Movement
Learning to feel our own discreet, hidden away pelvic floors is a thing! We can do it from the outside with our clever hands and brains, breath and movement. It's our brilliant and amazing bodies finding how to move with ease, support our organs, breathe in many different ways, manage pressures inside our bodies and in daily life. All of it! It's super simple and here's how. Start by standing up and reaching down with your long, middle finger to feel your very own anus from the outside; the "external anal sphincter" is her full name. Studies show us that feeling with your mind's eye and with your finger is the best indication of the activation and release of your pelvic floor. You can use both hands or just one hand (which is easier). Hold your middle finger on your anus and let your index and fourth finger rest on either side of your anus. They're helping you feel the action! Now…the action:
Would you like a different view/feel/idea? Let your finger go a little north of your anus and rest on your tailbone or coccyx. It's the tiny triangular bone at the base of your spine; it's an attachment point to your anus and other pelvic floor muscles. See the tiny bone angulated forward on the picture? It has a big role in pelvic muscle function! Now….the action:
Homework….ask yourself:
 Pelvic Pain conditions are so common.....1 in 10 Canadian women have endometriosis, 1 in 10 Canadian women have always experience painful sex (primary dyspareunia).....and that's just the tip of the pelvic pain iceberg. There's painful urination, postpartum vestibulodynia, postmenopausal genitourinary syndrome, evacuation disorders of the bowel, proctalgia fugax......many, many more.
But there is a commonality in many pelvic pain syndromes (with the HUGE proviso of "please see a pelvic physio, get diagnosed and proceed with a bespoke programme) that are summarized in this self care document. Self Care for Pelvic Pain Conditions Mar 2022 Goal: enjoy life's activities that stay as sub-threat (no grizzly at the door), non-nociceptive (always staying pain free), fun (laughter, silliness and joy) and fulfilling function (meaningful work, play, restorative activities). Where we start: You are normal. You're not broken. Everyone is different. You are unique. Where we're going: You're in the drivers seat; you're in control. The pain is happening to you (yes), but you can control the volume and choose your response (YES). Pain is part of life (inevitable) but suffering is optional (you can change the story of the pain you've experienced). How we do this: We help you learn to calm your pain response. Firstly, you calm the pain response down, then you build yourself up. Self Compassion takes three roads:
Control your thoughts:
**Specifically effective in reducing pelvic pain as the pelvic floor muscles + jaw muscles are the first and most active muscles to respond to anxiety or stress or fear or pain (or all)** 3 Good Things Practice: write down the 3 good things that happened today (Keep it simple: You woke up safe and warm in your bed, You had coffee, You can take time to write 3 things down) within 3 minutes Movement: Balance out your movement and rest, leaning towards shorter more frequent rests and consistent, happy, gentle, calm movement through your day
Food You Eat/Nutrition: evidence based food choices to reduce inflammation and influence pelvic pain, All evidence points to a healthy, whole food, organic, plant based diet ("Real food, Mostly plants, Not too much").
Self medication with opiods, alcohol, cannabis - have a look at your short term use and long term goals….do they match up happily? Are there other options that are non-medicative, non-addicting, narcotic-free? Yoga: classes at The Yoga Room with Barb Minichiello, Gail Thompson or Stephanie Derraugh and/or online with Shelly Prosko, Part A for quieting, Part B for activating on Vimeo (clientdiscount10 for 10% discount) **Twice weekly for one hour over 6 weeks is effective in reducing pelvic pain on long-term studies** **Three poses specifically help: Legs up the wall, reclining bound angle (fish), Savasana (corpse)** Sleep: good, consistent sleep reduces your pain perception and improves your pain resilience, ask for sleep hygiene handout/help. Skin Support:
Do a monthly vulvar and vaginal assessment with a hand mirror (ask for the handout) of your skin condition, your movement with breath, bearing down and closing/lifting. **Property of Full Circle Physiotherapy, not to be reproduced without permission** Joanne Gailius, BSR, PT/OT Physiotherapist Full Circle Physiotherapy C2 - 1204 NW Blvd. Creston, BC Ph 250-254-3494 Fax 1-855-655-5281 [email protected] How to Fully and Completely Empty Your Bladder or How to Void Well (pee, tinkle, wee, widdle, micturate, go to the loo……) First, what is normal, healthy voiding for an adult woman or man? Think about each of these statements and ask yourself, "Does this describe me?"
Now…..when you arrive at the toilet, there are some tricks to keep in mind.
Joanne Gailius, BSR, PT/OT Physiotherapist Full Circle Physiotherapy C2 - 1204 NW Blvd. Creston, BC Ph 250-254-3494 Fax 1-855-655-5281 [email protected] Mar 2020  Topic of the week at Full Circle.......post menopausal women in their 60s, 70s and 80s
working hard, busy harvesting in this agricultural valley and frustrated! In pain! Pushing too hard! Not coping, not sleeping, not restoring. This blog is a loving reminder that after our bodies are no longer supported by estrogen, we aren't as physically strong as we once were BUT even moreso, our endurance will have waned somewhat. There are some habits that will bring us joy in doing those meaningful work, rest and play. Here are my suggestions: 1. Jot down your list in pencil, then prioritize. What 3 job actually need doing today? Which ones could wait until tomorrow or tomorrow's tomorrow? 2. Know when you have the most physical, emotional and relational energy. Match the job to the time with some cleverness. 3. Stay ahead of your endurance dips. Plan a wise, intentional, constructive 15 minute rest mid or late morning and repeat that in the afternoon. Don't wait until you're at the over and out stage! You'll know that you're becoming brilliant at this when you feel pretty lively in the early evening and have the energy to enjoy some fresh activities when the sun is going down. 4. Support your sleep. Get boringly attentive to the same time, the same place, the same room, fresh air, warm bed, comfortable sleeping duds, no tech in the room (use a non-cellphone alarm)......think of when you were desperately trying to get your babes to bed and treat yourself with the same brilliant sleep support. 5. If you enjoy a daily glass of wine, have it at lunch rather than dinner or evening. Wine can create a pancreas-induced awakening in the wee hours. 6. Awaken with energy......you'll know that you're doing all of the above well when you awaken with energy, not ache and pain and dread. 7. Go for a walk. Those big muscles that move you through space (your gluts) are made for the job. Enjoy a walk daily. Breathe in deeply and stand tall at each telephone pole that you pass, letting your arms swing with each step. Enjoy the freedom of movement, the place that we get to live and the beauty of the onset of autumn. 8. Make time for something that you truly enjoy. Knitting? Reading? T'ai Chi? A phonecall with someone that you miss? An email or an old fashioned letter? 9. Most Importantly - Know your priorities, moderate your expectations and have respect for your age and stage. You're one of the lucky ones who is here with all the wisdom that the years have brought. Some self-compassion and self-care (not just self-soothing.....a pedicure and manicure are wonderful, but self care is the practice of employing daily habits that provide you with optimum health and joy) go a long way. Take care of yourself. 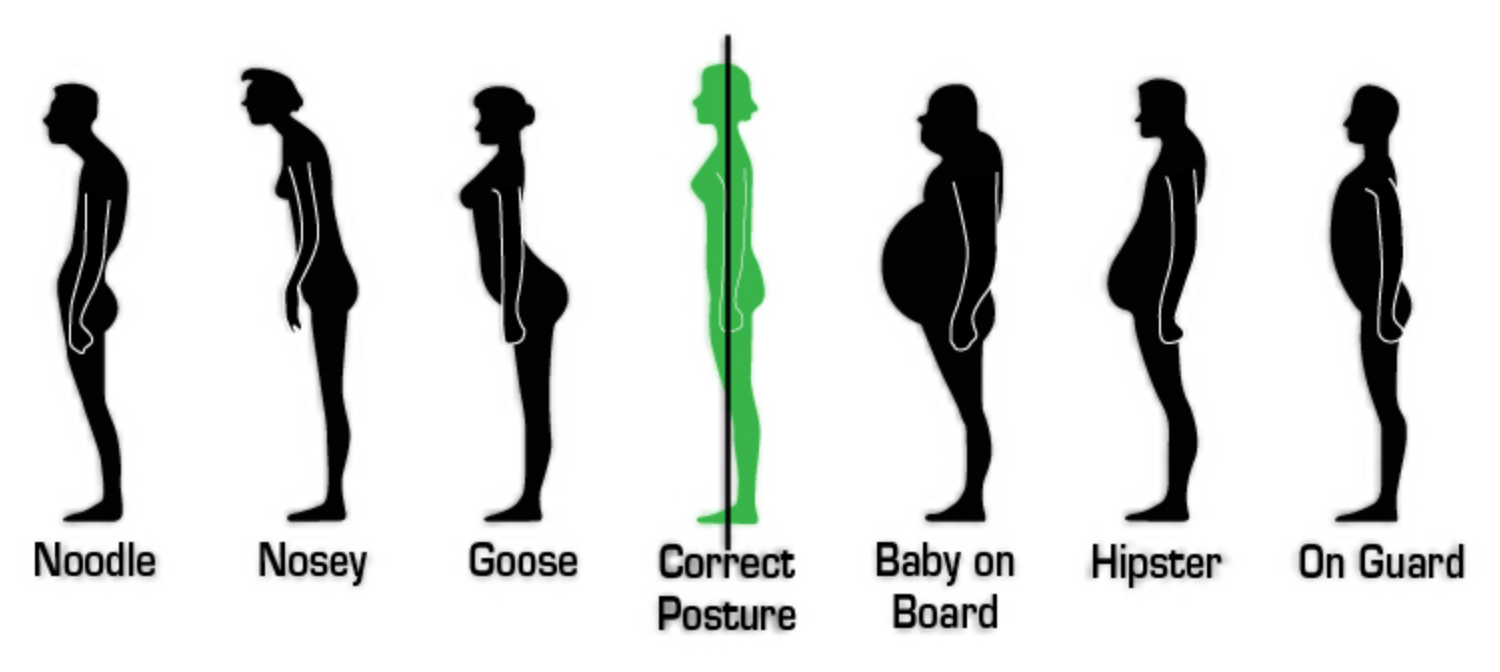 As the days are shortening, the evenings are having a sense of chill and we're harvesting tomatoes and peppers.....we begin to see the glimmers of summer's end. "Unprecedented" describes the summer of 2020 in every way. It's been a summer of constant change, resiliency developed, losses noted and a deeper sense of home for so many of us. No traveling? You've stayed home, found your place, your town, your city. Not visiting restaurants? You've cooked at home more, enjoyed takeout, eating in the park, shared meals with family more often. Not going to the gym, pool or ice rink? You've walked, biked or just rested. Or???
Interesting times. This is a short blog, a simple nudge to check in and take care of yourself. Check in with the human in the mirror. Notice how you're feeling, how you're thinking, how your body is responding to today and all it has brought to you. You don't have to begin to journal or meditate. Checking in with your one and only home, the body you inhabit is a gift to yourself. Our body "keeps the score", noticing all the experiences, interactions, life habits that we experience every day. Are you holding tension in your shoulders? neck? pelvic floor? hips? feet? What would it feel like to let that go? Maybe tighten up your tight area more....more..........more. Then release! Is that different? Is your posture restfully letting gravity pass through you when you're standing up? Or are you a "bum tucker", "chin poker" or "sloucher"? Begin at your sit bones (in standing).....rock them back and forth with your breath, then let them release just when they're pointing straight to the ground. Feel them! They're an amazing pair of dense, thick, strong bone that is the centre of your pelvic floor and your sitting destination in the chair. Hold that. Then lift your sternum (breast bone) up to the sky. You'll feel your braband lift off your front ribs, your mid spine activate right where your bra does up, your shoulders rock back and settle and feel an urge to take a brilliant, nutritious deep breath! Hold that. Finally, tuck in your chin towards the back of your head, not tipping forward, simply making a wee double chin. You might feel an urge to clear your throat or swallow. Hold that. Now notice how that feels. Look forward. Feel tall and strong. Really Strong!!! Gravity is passing directly through you, through the curves of your spine that provide you with spring-like responses to movement, through your strong, dense cortical bone and your balance will be dynamic and spunky. There is no perfect posture. Each of us is built differently, has had different experiences in life and does different things with our body each day. But you can enjoy ease in your body by taking time to check in and find ease-filled, gravity-enhanced, respiration-supported posture and movement through your day. When you notice that life feels heavy, that losses feel cumulative and "life as it was" feels distant, find your strong posture, your gravity defying self. Breathe fully. Balance well, Stand and walk with ease.  The second chapter on men's pelvic stories is a more specific look at how men (and those who love them) can work through pelvic challenges, focusing on prostate cancer, surgery and treatment. The first chapter talked about the pelvic problems that a man may face. The good news is that with pelvic physiotherapy and a solid commitment to follow through with the work at home both before and after surgery and treatment, complete resolution of both leakage and impotence is possible. Each man will have varying severity and duration of these physical side effects and they can lead to a much reduced quality of life. You can rewrite your story with help.
The protocol that is described here leans heavily on the brilliant work of Jo Milios in Australia, a pelvic physio devoted to men's pelvic health and aided by over 3000 men who have had radical prostatectomies. Men who followed this protocol had much less leakage, much reduced duration of leakage and a much improved quality of life throughout their recovery time. Even more convincing is the statistic that 1 in 6 men had no leakage whatsoever! For 4 - 6 weeks prior to surgery and resuming immediately after surgery, men are taught the following protocol: six times daily, in a standing position, two exercises are performed. The first is 10 fast twitch (or speed 'ems) maximal (full on!) contractions and releases. These are followed by 10 slow twitch (endurance building or hold 'ems) contractions, holding each for 10 seconds with a 10 second relaxation time between each contraction. It's important to find "the right muscles". Try this: squeeze the front passage as if you're stopping the flow of urine, then lift your testes and retract the penis. Doing these exercises in standing is important as this is the position in which most men leak. With your pelvic physio, you'll learn awareness of which muscles activate correctly, then how to release fully and more! The importance of "pre-hab" or beginning training prior to surgery can't be reinforced enough. The time between biopsy/diagnosis and surgery is a time to begin learning about your pelvic function, strengthening and releasing. Bladder control (voiding with control and fully 6 - 8 x daily or learning to do so) and a happy bowel really make a difference as you head into the choppy waters of surgery and treatment. Jo's research has shown that men respond very well to the improved physical control of their waterworks and sexual function with this help, but additionally they are emotionally and relationally so much stronger! Her goal is to improve the quality of life for all undergoing prostate cancer diagnosis, surgery and treatment. Let's get specific....one appointment for assessment/training is sufficient to help you begin. Palpation can be done externally in most cases. Your important three muscles that control your urine, the trio that you need to learn to turn on and off and strengthen are called the external urethral sphincter + bulbocavernosus + puborectalis. Sometimes that pesky external anal sphincter gets dominant and you need to learn to teach it to quiet down. Once you've found these muscles, you'll move onto working in synergies, becoming powerful (for coughing and sneezing), strong (for sit to stand and lifting), having endurance (for standing and walking), improving the quality of contraction/lifting of the pelvic floor as well as improving release/relaxation in order to support the next contraction. The toughest bit? Fatigue. Standing upright will fatigue the system and that fatigue may worsen as the day progresses, causing leakage to occur. Many men will have overactive muscles that need to learn to release and NOT exercise at first (called pelvic downtraining), some men will vary  When I write about women's health, oncology (cancer related) and pelvic physio, it's a logical to assume that it's only women that we pelvic physios assess, treat and talk about. This is the first in a series of articles that will introduce you to the challenges that men face in their pelvic region, despite "being absolutely mortified to be discussing their private parts" (to quote Dr. Jo Milios, our lead teacher, a brilliant physio who had set up a non-profit organization in 2012 in Australia called PROST! Exercise for Prostate Cancer Inc.). Her passion is to educate all of us so that the everyday man on the street has better health outcomes and a much longer life.
Pelvic physiotherapy for men addresses loss of function in the pelvic region including prostate cancer pre-hab (prior to surgery and other treatments) and rehab, pelvic floor muscle dysfunction, urinary incontinence, painful urination, recurrent bladder infections, urinary frequency, bowel dysfunction, erectile dysfunction, chronic pelvic pain syndrome and Peyronie's Disease (a crooked or bent penis). Let's begin with the prostate. The prostate gland is a walnut sized donut shaped gland found right under the bladder and wrapped around the urethra (urine tube). Its job is to produce most of the fluid that makes up semen. The prostate can become inflamed (prostatitis, acute or nonbacterial) or enlarged (benign prostatic hyperplasia). Enlargement of the prostate doesn't mean it's cancerous and is usually noticed after age 40 during a regular doctor's visit. Prostate cancer is the most common cancer in North America and accounts for 11% of all cancer diagnoses in BC men; 1 in 9 males is expected to develop prostate cancer in their lifetime with 89% of them being over the age of 60 when they are diagnosed. There are some well known correlations (not causes) that may raise a man's risk of developing prostate cancer, including aging, family history, high levels of testosterone, being overweight, not exercising regularly and a poor diet. Large studies have shown that there is no correlation between having a vasectomy and prostate cancer. Yet again, Grandma's sage advice to exercise regularly, eat real good and maintain a healthy weight (for all cancers!) are actions that you can take to reduce your risk of developing prostate cancer. Your doctor (GP or urologist) or nurse practitioner may do a DRE (digital rectal examination) to palpate your prostate or you may have a PSA (blood test) to measure how much of a specific antigen is in your system. If you notice changes in your urination (stuttering flow, slow stream, painful, frequent, dribbling/double voiding, feeling the urge to bear down to start or finish, urge or loss of control, increased night time voiding or blood in your urine and/or painful ejaculation), please tell your doctor. Even though it's difficult or embarrassing to open up these conversations, your healthcare professional will want to know, will have had these conversations before and will make you comfortable sharing your story. Tell them! We pelvic physios become involved with men going through prostate surgery because most men (99%) will experience incontinence and erectile dysfunction. One of the prostate's secondary jobs it to support the bladder and to give neurological support of continence through the autonomic (involuntary) nervous system. The Cavernosal Nerves, responsible for erections, are wrapped around the prostate and they're usually damaged or removed in the process of the surgery. Each man will have varying degrees or severity and/or duration of physical side-effects of the surgery but please know that each man will generally improve over time. With pelvic pre-hab and rehab, complete resolution of both continence and sexual function is possible. It's all about restoring wonderful function and quality of life while reducing anxiety and depression, penile fibrosis and shrinkage and stopping the development of Peyronie's disease. Most importantly, men and partners who love men, talk with your doc if your experiencing pelvic dysfunction. In part 2 of this series, I'll share Dr. Milios' well researched brilliance after seeing >3000 men with radical prostatectomies, showing that, by using her protocol, men had less leakage (in amount and duration) with 1 in 6 men having no incontinence at all! |
Archives
January 2024
Categories
All
|

 RSS Feed
RSS Feed
